iGATuBioBank [82146] Jennifer Joy Brenley Nyhof
Healthy Whole Blood Donor Jennifer Joy Brenley Nyhof
Frozen Plasma [constituents] June 18 2024
| Cell Type | Number of Cells (/mL) | R.I. (/mL) |
| C.D.9+ | 4000 | 1 |
| C.D.90+ | 8520 | 8 |
| C.D.1+ [omnipotency] | 436 | 0 |
| Biochemistry | R.I. (mg/dL) | |
| Total Protein (mg/dL) | 85360.0 | 3631.0 |
| Albumin (mg/dL) | 0.36 | 0.05 |
| Globulin (mg/dL) | 63.6 | 1.36 |
| D-Dopa [D-enantiomer](µg/mL) | 4.31 | |
| Immunology | units / mL | R.I. | ||
| IgD | 4.32 | IgA > IgG > IgD > IgE > IgM | ||
| IgA | 3.31 | |||
| IgG | 2.16 | |||
| IgG1 | 3.60 | |||
| IgG2 | 2.70 | |||
| IgG3 | 1.60 | |||
| IgG4 | 9.60 | |||
| IgM | 3.12 | |||
| IgE | 1.61 | |||
| Comments: IgD-IgA dimers noted. | ||||
R.I. [Reference Interval]
C.D. [Cluster of Differentiation]
Ig [Immunoglobulin]
PBSC [Peripheral Blood Stem Cell] are many and include those denoted as C.D.90+ and C.D.1+ [omnipotency] in table format above
Jennifer Joy Brenley Nyhof, whole blood donor, did NOT undergo or accept G-CSF treatment administration at ANY time and has never done so; G-CSF = granulocyte-colony stimulating factor
Roitt, Ivan M., Delves, Peter J., Martin, Seamus J., and Burton, Dennis R. 2017. Roitt’s Essential Immunology. Thirteenth edition. Wiley Blackwell. John Wiley and Sons Ltd. Oxford, United Kingdom.
Hunt CJ. Cryopreservation of Human Stem Cells for Clinical Application: A Review. Transfus Med Hemother. 2011;38(2):107-123. doi: 10.1159/000326623. Epub 2011 Mar 16. PMID: 21566712; PMCID: PMC3088734. https://pmc.ncbi.nlm.nih.gov/articles/PMC3088734
In-vivo production and manufacturing (inside the human body) of d-DOPA the d enantiomer of DOPA the enzyme and neurotransmitter and hormone, as well as stem cell omnipotency according to the cluster of differentiation CD classification system, in Jennifer Joy Brenley Nyhof (this writer) is greatly enhanced by involuntary Val Salva maneuver phenomenon and Cheyne-Stokes breathing respiration patterns at rest and during active rest and during mild to moderate to strenuous exertion. Let me tell you a bit more about how I do it. The predominant pattern of my breathing respiration at rest is 2 sighs followed by 1 end expiratory hold lasting 2 seconds followed by 1 sigh followed by 2 end inspiratory holds lasting 1 second each. During mild and moderate physical activity equivalent to a 1, 2, 3, 4, 5, or 6 on the rating of perceived exertion RPE scale, the predominant pattern of breathing respiration is 1 sigh followed by 1 end expiratory hold lasting 2 seconds followed by 2 sighs followed by 2 end inspiratory holds lasting 1 second each. During more strenuous physical activity, equivalent to a 7, 8, and 9 on the rating of perceived exertion RPE scale, my predominant breathing pattern is 4 sighs followed by 1 end inspiratory hold lasting 1 second followed by 1 sigh followed by 2 end inspiratory holds lasting 1 second each. During very strenuous physically active exertion, equivalent to a 10 on the RPE scale, my predominant pattern of breathing is 1 sigh followed by 2 end inspiratory holds lasting 2 seconds each followed by 1 sigh followed by 1 end expiratory hold lasting 1 second. Intermittently applied end expiratory Val Salva is performed during tasks requiring pushing or pulling objects to or away from my body, such as when lifting a suitcase off of the ground. Intermittently applied end inspiratory Val Salva is done when I sleep once every 41 seconds and it lasts for 2.391 seconds on average each time I do it. I commonly end expiratory hold my breath when I’m just thinking. This supraphysiological process and pattern of breathing respiration facilitates cellular omnipotency stem cell progenitor reversion and differentiation, as well as d-DOPA production, and it can be confirmed and verified with spirometry / capnography.
and here is some resource material that has to do with my general knowledge and expertise in producing and creating sound within the infrasound infrasonic range of hearing and feeling sound waves and this is known as A.O.V.I. T.echnology and I do this with my own vocal cords and mouth and diaphragm and oropharynx and nasopharynx and eye orbit and lungs with good breath control
| A.O.V.I. [aural, oral, and visual imagery with tactile enhancement] T.echnology | |||
| [frequency] [f][Hz] | [decibel] [dB][range] | [notes on sound production] | [perception]/[effect]/[outcome] |
| [perceived as pitch] | [perceived loudness] | [receiver/recipient of message] | |
| Physiological resonance 3 – 8 Hz [see further] | |||
| 1.0 Hz | +5.0 dB – +20.0 dB | sitting, standing (nearly) completely still; peak expiration; breath hold; slight mouth and jaw movement [nasopharynx]; [melody][harmony][spoken word] | calm |
| 5.0 Hz | +10.0 dB – +20.0 dB | standing, sitting, lying down / sleeping [supine, semi-supine] [per R.E.M. cycle]; with narrow impedance; on very slight exhalation [open glottis][oropharynx][mouth]; [melody][harmony][spoken word] | anti-nausea, anti-emetic, analgesia, euphoria, attractiveness, orgasm quality [climax], vasodilation, improved speech pattern and articulation, to be likened by all |
| [low G][16th octave] | |||
| 6.0 Hz | +20.0 dB | lying down / sleeping [supine][per R.E.M. cycle], transition [inflection] to 5.0 Hz; [melody][harmony][spoken word] | nice, content, happy [feeling/emotion] |
| 6.0 Hz | +40.0 dB | lying down / sleeping [supine][per R.E.M. cycle], transition [inflection] to 20.0 Hz; [melody][harmony][spoken word] | orgasm [climax] |
| 10.0 Hz | +10.0 dB | standing tall, sitting tall, neck held in dorsoflexion 10° off horizontal; with projection throughout respiratory phase; [melody][harmony][spoken word] | excited, alert |
| 12.0 Hz | +10.0 dB | standing tall, sitting tall, neck held in dorsoflexion 20° off horizontal; with projection throughout respiratory phase; [melody][harmony][spoken word] | happy, excited, energetic, satiety, social awareness, spatial awareness; [perpetuated over proceeding 1 minute] |
| 20.0 Hz | +25.0 dB – +40.0 dB | standing, sitting, neck held in normoflexion 0° off horizontal, with projection throughout respiratory phase, further on exhalation; [melody][harmony][spoken word] | increased focus, attention to detail, observational capacity, motivation; [1 minute to initial effect][perpetuated over proceeding 5 minutes thereafter] |
R.E.M. [Rapid Eye Movement]
Hz [Hertz][S.I. Unit of Frequency]
dB [Decibel]
With acknowledgement and reference to Morton and Ohlbaum. August 1976. Mechanical Resonant Frequency of the Human Eye in Vivo. Aerospace Medical Research Laboratory. Aerospace Medical Division. Air Force System Command. Wright-Patterson Air Force Base, Ohio, 45433. Attn: A
and now I will share more information about scientific research and biobank biobanking in context of my work as the Core Facilities Manager at the iGATuBioBank
for the human species, saliva salivary secretions oral cavity fluid here is some information about biochemical composition
- an increase in the rate of saliva production towards the upper bounds of within the physiological range of normal, akin to slight or mild to moderate hypersalivation figuratively speaking, leads to the following changes in composition of salivary secretory fluid within the oral cavity
- water content remains constant within physiological tolerance bounds at 97.817% pure water H2O
- sodium Na2+ content increases by 3 – 5 mEq/mL
- bicarbonate H2CO3 content increases by 1 – 2 mEq/L
- salivary pH increases by 0.005 while blood pH decreases by 0.02
- potassium K+ decreases by 3 – 4 mEq/mL
- ionized calcium Ca2+ decreases by 1 – 2.42 mmol/L
- bound phosphate H2PO4 decreases by 1.376 mmol/L at max
- chloride Cl- decreases by 1 – 2.543 mEq/mL
- urea decreases by 3.219 mmol/L at max
- total protein [albumin and globulins together] decreases first by 3.19 g/L and then increases by 1.29 g/L from the decreased value at max
- albumin increases by 1.294 g/L at max
- globulins decrease by 0.296 g/L and then increase by 1.987 g/L from the decreased value at max
- the predominant glycoprotein as a component feature of physiological saliva is glycosylated end product methylglyoxal MG and substituted methylglyoxal MG products and their derivatives. The concentrations of methylglyoxal MG and substituted MG products and their derivatives in this physiological hypersalivation situation we are discussing comparatively speaking, increases from 8.191 g/L at relative baseline to 9.1829 g/L at max
P.S. this is my notebook
- the word research and doing research is not synonymous with and it does not equal and it is not the same thing as “testing things out on animals” and emphasis is placed on learning and knowing words like retrospective prospective cross-sectional literature review and meta-analysis when it comes to study design and understanding what a clinical trial is and what it is not and what it means to apply or NOT apply a treatment to anyone in a group of participant subjects like maybe none at all and knowing what it means to make observations passively like watching things happen as time goes by and making notes on them
- substrate / NRG / oxygen limited {or excess} local environment
- cell “escapes” cell cycle control checkpoint, altered enough so the cell doesn’t die but results in a change in the protein / receptor on the plasma membrane
- possibly recognized as a foreigh antigen by MAC/Dend/APC; allosteric to MHC1 / or sterochemistry restricts/permits recognition of self
- an error in: transcription (nucleus) / translation (rER / ribosome) / post-translational modification (golgi)
- warning signal / conserved vs variability ? / altered surface marker that is NOT MHC1 (non-MHC1) expressed by damaged / altered / abnormal cells
- utility?: if change / error (ex. methylation vs phosphorylation) manifested in a way that could be recognized with higher affinity / specificity by the APC / coupled with T-cell recruitment and destruction / [also humoral/complement]. What would that mean?
- potentially, a mechanism for early identification and destruction of pathogens / pre-neoplastic to neoplastic cells
- primary, secondary, and tertiary prevention of infectious disease and neoplasia
- identifying / isolating APC antigen presenting cells from indivdiuals with such an ability / higher affinity / higher specificity for a potentially conserved warning signal trigger of foreign antigen all of them / ~ you can probably only get away with so much “error” before the cell is non-viable –> apoptosis / lysis – there are a finite number of ways to make something a bit wrong and still work
- #1 82146 / validation
- abnormal tissue
- KO knock out MHC1 major histocompatibility complex human leukocyte antigen HLA9
- Macrophage / dendritic cell (+ biotin conjugated Ab antibody)
- IHC immunohistochemistry
- #2 Assay for altered protein / altered fxnal functional product that results from the alteration – electrophoresis / HPLC high pressure liquid chromatography / GC gas chromatography etc.
- +/- macrophage / dendritic cell (+ biotin conjugated Ab antibody)
- #1 82146 / validation
- identifying the limiting [or excess] conditions that incite / propagate the problem – to manipulate cells in and out of Go Re: disease control / return of differentiating potential / potency
- insert previous information with regards to microthrombus formation in terminal capillaries (afferent): [decreased oxygen tension / subtle hypoxia in supplied tissue beds]
Like Bone Marrow / Bone
Recall that platelets are the cell fragments formerly megakaryocytes that are nonhematopoietic cells (of the bone marrow and blood tissue)
Allogeneic ICM hESC (degree of differentiation?) +/- Autologous or Allogeneic Serum +/- Microbiome / build in situ human tissue bioteactor
4 layer device
- Deep Tissue contact layer – akin to fine strands (6-0 monofilament) of dissolving suture material, interlaced (woven) to form a permeable / porous mesh
laid on the wound bed, secured with sutures to the wound edges if practical / possible - and
- Autologous or Allogenic Serum (~ stability of patient, disease status, immune competence) admixed with ICM derived hESC stem cells. Qualities and characteristics of bone marrow (intraosseous) minus the RBC component.
- +/- the other side of the equation: what is apposed to the treatment site / environment
intrarticular – might be primary closure of incision
lymphoblastic neoplasia – abN abnormal cell population has a bone marrow derivative (have to be made in the bone marrow – headed down the blast -> cyte line before they get kicked out into peripheral circulation) – / somewhere during the process there’s a division / replication / something that takes then outside of normal cell cycle control – uncontrolled proliferation of immature / abnormal ex. B cells (in B-cell acute lymphoblastic leukemia, for example). Moreover, their existence / replication doesn’t just escape cell cycle control, it evades the process that should identify the cells as being abnormal and target for destruction (shouldn’t have been made [to escape], and they [the one’s the cells that form the tissues who aren’t listening to the cues] should have been destroyed if they were). Problem??: gastrulation (they’re in the wrong place (bone marrow / should have ended up in the liver, cell type) and don’t have the right stuff (receptor / communication strategy / ion-gated channel ), environmental exposure (the wrong stuff (ie. teratogen / toxin / signal) is in the right place (bone marrow / cell type)).
I think it’s naive to think that autologous CAR-T cell therapy alone will be the panacea. The cells were raised / bathed / learned in an environment that wasn’t conducive to trust / building relationships that had a positive outcome.
It’s a few things:
- recogizing the importance of local immunologically active tissue thymus spleen MALT etc. because we don’t always know the nidus / stimulus / exposure that starts the process down the wrong path
- more help than just wiping out everything (the kill et al. )- why isn’t anyone asking the rest of the patient to live? including the immunologically active parts and the microbiome.
- local and global strategies like the part and the piece and the person people patient
- the restart needs a restart / allogeneic CAR-T Cell therapy
- hESC –> down the road of hematopoiesis –> culture them in an environment so they respond and target for destruction the appropriate receptor on the neoplastic cell line. As a whole blood transfusion. Plasma will still have it’s role. Remember (meta)….rubriblasts have genetic material to start with
- concurrent whole blood transfusion CD47+ SIRPa
my ongoing randoms
- thymus (regression, lack therof); positive and negative selection of T cells; histology
- M1 / M2 / M3 / M4 / M5 macrophages / chimera / polymorphism / role of post-translational modification / golgi apparatus*
- erythoropoietin EPO / testicular tissue in human men males / neoplasia incl. treatment modalities / normal tissue / homology / hypoxia / kidney and exogenous – therapeutic vs doping scandal performance enhancing drug sports competitive athletes
- allogeneic CAR-T cell therapy / coupled therapy treatment / RBC [type – Ag presence / absence / RH factor / major / minor cross match – see charts available elsewhere on other people’s websites] N.B. oxygen tension / disparity / cell fragility
- HLA / major histocompatability complex 1 as in MHC-1 shift / drift / inter v intra-individual variability
- incidence and severity [outcome] of Type 1 hypersensitivity reaction following administration of natural colloids (plasma) = rare <0.001%
- early embryonic / fetal exposure to antigens [self, similar, and non-self], immune stimulation, and effect, incl theory Re: embryonic / fetal “drinking” and fetal “eating” after the placenta has formed and post-gastrulation via gut tube / mucosal associated lymphoid tissue M.A.L.T. and specifically gut associated lymphoid tissue G.A.L.T development / tissue – resident macrophages / lymphocytes / neutrophils / CD1+ stem cells = cord blood derived hESC
- embryology / eyecup re: retinoblastoma / gut tube / notochord / invaginations / outside becomes inside except gut tube where outside stays outside / extend to chondrogenesis / laying down bone from cartilage template re: osteosarcoma
- immune surveillance of mammary tissue / lactation {higher pH c.f. other tissue-associated fluid / above pKA of X?} v no lactation / blood supply / pH – ion trapping [relative charge across the barrier] / mechanical stimulation / local trauma / ability for effector cells to gain access / cell fragility / hormone / neurotransmitter / charge / mammary neoplasia incidence / prevalence during pregnancy – gastrulation / mammary tissue development of the fetus
- study design / quality / nutritional plane / content / laboratory animal model / resiliency / robustness / selenium / vitamin E / thiamine / folate etc. / confounding variables
- cellular injury and cellular repair vs you’re doing it wrong / keep going when you shouldn’t ie. from the damaged inferior quality cell’s perspective with broken damaged genetic material it keep dividing and it should die by programmed cell death apoptosis / stop when you could keep going ie from the normal healthy cell’s perspective it doesn’t divide to fill a void when a void is there and new cells that form the tissue are needed sometimes desperately / ds vs ss double stranded vs single stranded breaks problems genetic material DNA RNA / “resolution” DNA pol ; RNA-dependent RNA polymerase human origin / transcription-translationomics
- dispase / separation of keratinocytes from underlying dermis / refer back to scaffold / Re: making ECM / articular surface / bone marrow – refer back to making bone from cartilage – germ layers / gastrulation / the right thing in the wrong place / the wrong thing in the right place / signal recognition / migration – the right time / the wrong time / the midline / refer to invagination / OSA osteosarcoma / RBA retinoblastoma — RPE retinal pigmented epithelium / MC; divergence / A.L.L. acute lymhoblastic leukemia –> learning / memory see self v similar v non-self (plasmacytoma / B cell / T cell) need for healthy B cell population – hyperimmune serum / plasma / whole blood / monoclonal / polyclonal gammopathy / therapeutic potential of the product of a productive “problem” –> knock out
- passing Go for $200, not passing Go for $200 [the stimulus / inhibition / activation / suppression] for entering and exiting Go re: cell cycle phases like M / G / cell cycle arrest
- the lac operon – glucose / lactate / other factors / transposable elements / transposons / TMV tobacco mosaic virus and the replication competent vector in context / lactobacillus thio-sulfur chemistry – gold extraction technique like ore precious metal / lectin / concavalin A biochemistry for good not evil including industrial applications / henderson hasselback equation is important here pKa 7.291 and pKa 7.3817 look these 2 up those of you reading this
- Tobacco Mosaic Virus TMV / bionanotechnology – alternate energy / leaf biochemistry – oak tree / electrolysis / gentle electroporation / battery / [galvanic] cell / electrode / lithium / nickel / cobalt / cadmium / land reclamation / bioremediation
- rheumatoid arthritis RA / dietary component contributing factor to disease / Vitamin D3 > 10,000 I.U. once daily sourced from a reputable credible supplier and a diet or supplement that is pharmaceutical grade / improvement in clinical signs after 4 days / resolution of joint space pathology via MR imaging in 1 day
- psoriasis / dietary and environmental component contributing factors to disease / Vitamin D1 > 10,000 I.U. once daily and Vitamin C > 1000 mg once every 48 hours sourced from a reputable credible supplier and a diet or supplement that is pharmaceutical grade / environmental contact with bees is protective [p=0.001]
- kidney stones / dietary component contributing factor to disease / Vitamin A < 1000 I.U. at a time is needed in terms of consumption at once [spaced apart by 2 hours or more] / Vitamin D1 > 10,000 I.U. once daily maximum / Vitamin E > 1000 microgram mcg once daily maximum / Vitamin D3 > 10,000 I.U. once daily divided if possible / Vitamin B6 = 100 micrograms mcg once daily / all sourced from a reputable credible supplier diet or supplement that is pharmaceutical grade / note the white potato in terms of consumption*
future work for good
In-vitro diagnostic test / Tissue Factor [Factor III] assay: hypercoagulability / thromboembolic disease tendency
96 well ELISA enzyme linked immunosorbent assay and the results are to be correlated with:
viscoelastic methods rotational thromobelastography TEM for modelling hemostasis and fibrinolysis, currently used / other available measures of primary and secondary hemostasis [ex. PTT] and biochemistry / hematology parameters including sedimentation rate, clinical correlation,
in context of acute or chronic disease / comorbidity diagnosis and management and
effect of pharmacologic intervention
- note sensitivity of current assays for Tissue Factor [Factor III]
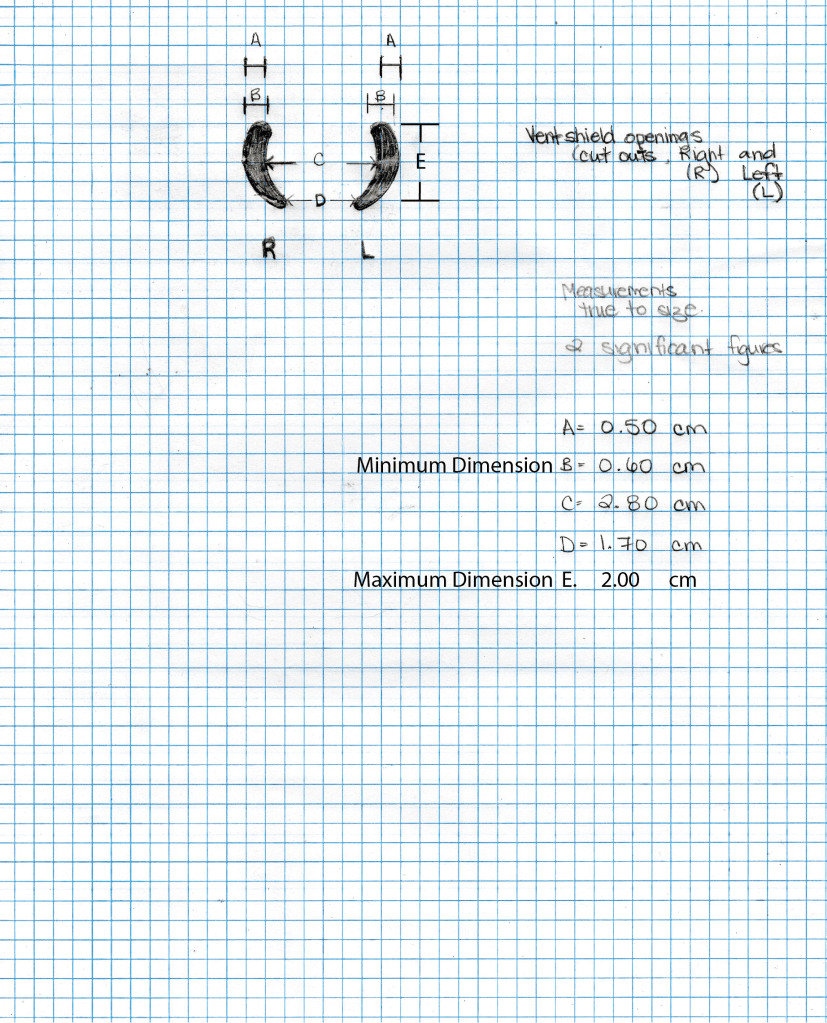
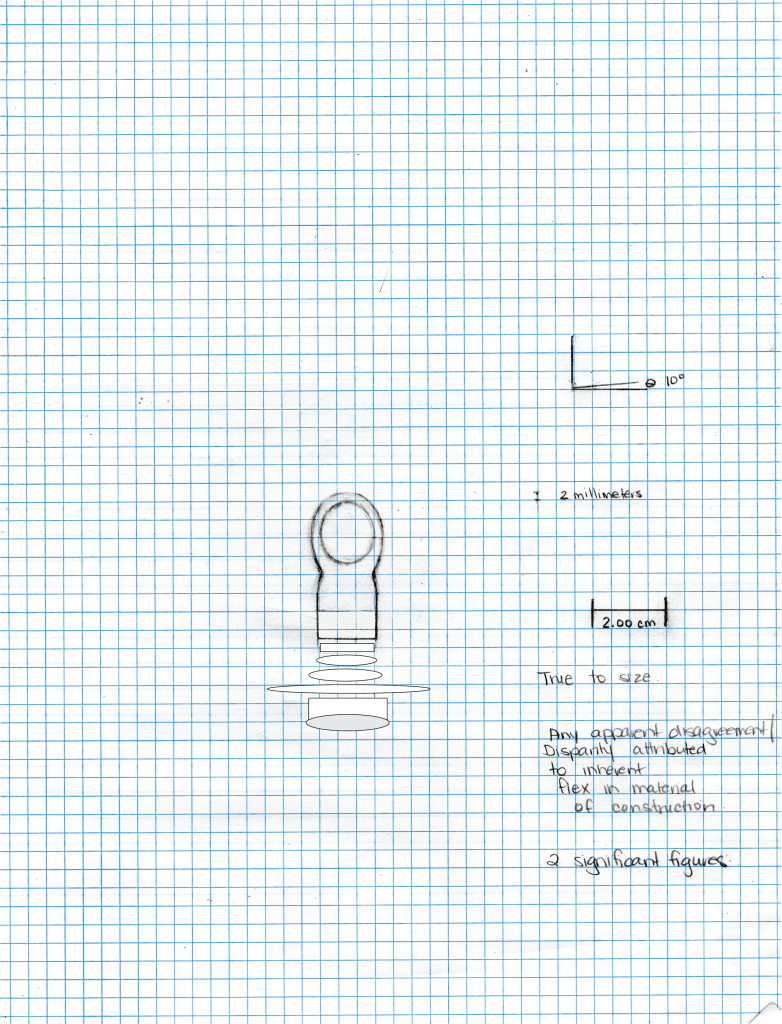
USPTO patent 18-062936 a novel pacifier-type device system of oral and transmucosal therapeutic agents [vaccine biologic pharmaceutical industry] held by Dr. Jennifer Joy Brenley Nyhof with emphasis added in context of the widely available oral cholera vaccine for human infants and mucosal immunity cross protection 31 years in vivo long lasting*